Melissa: I'm Melissa Harris-Perry. Welcome to The Takeaway.
One person dies of a fentanyl overdose in the US every seven minutes. Fentanyl kills more people than car accidents or gunshots or death by suicide. For people ages, 18 to 49 fentanyl overdose is the leading cause of death and some people have no idea they're even taking it. How did we get here?
Part of the answer lies in the potency of fentanyl. Developed over 60 years ago to treat those suffering from unusually excruciating pain, 1 milligram of fentanyl is equivalent to 50 milligrams of heroin or 67 of oxycodone. Just 2 milligrams can be deadly. A classic box explainer from 2017 tells the story of the Fentanyl crisis.
Explainer: First, Americans got hooked on prescription painkillers. Next, addicted users moved on to more potent drugs like heroin. Now, an increasing number of Americans are overdosing on an even more powerful opioid.
Melissa: This isn't just a story about individual users, there are policy implications. A well-meaning crackdown on US opioid manufacturers made prescription painkillers suddenly harder to get even as millions were already addicted.
Speaker: I'm deeply concerned about the challenge of illicit drug trade. First, I fully understand that when there's demand, there will be supply, and the United States of America is implementing a comprehensive strategy to convince our people to stop using illegal drugs.
Melissa: With demand high and supply diminishing, illicit drug cartels stepped into the gap. Traffickers that for decades relied on expensive plant-based drugs such as heroin, cocaine, and marijuana were now using chemicals in makeshift laboratories to manufacture fentanyl, and it was cheap, really cheap. By 2016, the CDC pressed the Obama administration to declare fentanyl a national public health emergency. While the administration considered the request, it chose not to act. A year later, the Trump administration's solution was build a wall on the US-Mexico border.
Trump: We will work, we will pray, and we will fight for the day when every family across our land can live in a drug-free America.
Melissa: In October, the Biden administration announced a multi-prong strategy, which includes putting a stop to inappropriate prescribing of opioids, expanding medication-based treatment, and improving support for people recovering from substance abuse disorders. Now, it sounds hopeful, but experts say that the rapid surge of synthetic drugs has created a new frontier in the drug war. On May 10th of this year, the DEA announced their first-ever national fentanyl Awareness Day.
Speaker: Please be sure to talk with your friends and your family about the dangers of this deadly substance. Together, we can save lives.
Melissa: We wanted to understand more about the ways that American law enforcement has thought about and addressed the fentanyl crisis over the past decade. I had a conversation with retired Assistant US Attorney Sherri Hobson. Hobson spent much of her career in San Diego, an epicenter of the fentanyl crisis.
Sherri: I've spent the last 30 years of my career as an Assistant US Attorney in the Southern District of California. Back in 2015, several agents came to me and said, "Sherri, we're seeing fentanyl at the border." At that point, I knew fentanyl was prevalent in certain parts of the country, namely Ohio, where there were a number of fentanyl deaths so we started with six cases in 2015. In 2016 that jumped to 19 and by 2017, it was 75. It was escalating but in the meantime, there was this push by the Trump administration that the wall was going to stop the flow of drugs and save America.
The problem was that that was not true. What was happening was 85% to 90% of the drug seizures that we were seeing at the ports, and this includes fentanyl, it includes methamphetamine, cocaine were at the lawful ports of entry.
Melissa: Okay Sherri, unlike opium, fentanyl's synthetic. Can you help us to understand how that affects the ability of the drug to move across borders?
Sherri: Certainly. Fentanyl is synthetic, so you can make unlimited supplies. All you need to do is manufacture it in a lab, in someone's apartment, in a warehouse. For example, with methamphetamine, you generally need 5 kilograms of different types of chemicals to make approximately 1 kilo of methamphetamine. All you need is a tiny bit of fentanyl, and you could make a lot of fentanyl. Fentanyl was very different. I think one of the mistakes was that people were treating it like a regular drug and it's not a regular drug, because you just need a little bit to make a lot and the profit margin for fentanyl was so high for the traffickers.
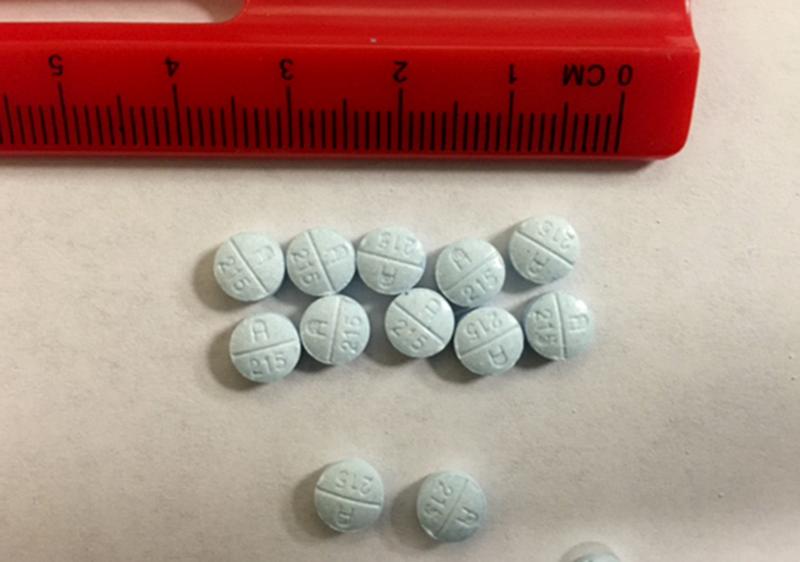
You could see how much drugs you have in your community, like how much fentanyl you have in your community based on how much the traffickers are selling it for. When we started and we saw a blue pill that contained fentanyl, it was $20 $25. By the time I retired in 2020, it was down to 5 or 6. This was going to be an explosive problem for America because you had millions and millions of people already addicted to the pharmaceutical oxycodone. The traffickers saw that there were millions of addicts here in the United States. There was no treatment for these people.
There was treated maybe in certain areas, but people were looking for something. At that point, they turned to these blue pills. When we saw these blue pills coming through the border, I was like, why is it blue? Why is it M30? We know why because people were using it as a replacement when the pharmaceutical industry was reined in. This is back in 2015, 2016.
Melissa: Everything I know about macroeconomics tells me if I've got high demand that is inexpensive to make the product if the product and making it actually becomes a little less expensive, that I will never be able to control this problem. People will always want it, it will always be available. Are we past being able to do something about this?
Sherri: It's not a problem you can solve with a simple answer. I said this in 2017 at a conference, which is you can't arrest your way out of this problem. I'm not saying not to prosecute, but we can't arrest ourselves out of this problem. You can disrupt people's organization, but it's going to come back. I just know this from my experience as a prosecutor. I started my career doing 2-pound methamphetamine cases and my last trial was hundreds of pounds of meth and heroin and fentanyl, and that's over a 30-year period. I'm a very positive person but I'm also pragmatic.
Do you do treatment? Absolutely you do treatment. Do you do prevention? Absolutely you do prevention. I'm not optimistic. I think you have to understand the evolution of how we came to this point. Then I think you just manage the best you can.
Melissa: I've talked with some guests who have said that's right, people are going to do drugs and so what government policy should do is to ensure that they know what kind of drug they're doing so that they don't accidentally die of a fentanyl overdose. What government could do to intervene at this point is to allow testing kits. To decriminalize drug use so that people can use without fear of criminal reprisal and that maybe they would have a test strip so they could actually test their drug before they took it and know, is this cocaine or fentanyl? Is that kind of move one that you see as a potential road to solution, or will that also not get us to a safer public health situation?
Sherri: These are things that are important. In San Diego County, all of the sheriffs in the police department, they carry a NARCAN. I want to point out this issue because I think it's important for people to understand. When we first started looking at the fentanyl coming through the port in San Diego in 2015, '16, '17, '18, '19, they were all roughly 6% to 8% purity on the powder form. In other words, it was pretty consistent. What that means to me as a prosecutor is that it's generally one source because the purity is pretty consistent.
Now, I'm being told by a number of people, including chemists that it's all over the board. You could have 6% or 18%. That's a problem because what that means to me as a prosecutor is that there's more and more people that are making it. In other words, there's more and more people that are taking the fentanyl and making it into different levels. Once you start seeing the divergence of the purity level, that's a problem. I think people have to stop looking at it as the traditional drug because this is the only drug in my career where someone can take it for the first time and die.
You don't die from meth when you first take it. Methamphetamine abuses your body over a period of time. With fentanyl, you can take it the first time and die. We have to think outside the box and approach it differently, but you're not going to solve this problem. Meaning when they come out and say, "We had the biggest drug bus and it saved millions of lives." Well, that's not addressing the fact that you probably missed 90% of the drugs.
Melissa: Are there things that we're missing right now that if we turned our attention to, perhaps it wouldn't solve everything, but maybe it could at least save some lives, stem some of this problem?
Sherri: The other day I was asked this question and I said, you know what? I'm really sad. I'm just sad. It's just there is no one solution. You have to have people stop using drugs and educate them about what it is. Yes, the NARCAN is good, the testing is good, but you really have to go to the issue, the crux, which is traffickers are not going to make any money if you're not buying their drugs. That's really what it comes down to. I know this is hard for people to understand, but there is no one solution. It's evolved into a deadly situation for America.
Melissa: Retired Assistant US Attorney, Sherri Hobson. Thank you for taking the time with us today.
Sherri: Thank you for having me.
[music]
Melissa: Now take away, if you suspect that someone is experiencing an overdose, the CDC recommends the following. Call 911 immediately, administer Naloxone if it's available, try to keep the person awake and breathing, lay the person on their side to prevent choking, and stay with them until emergency workers arrive.
[music]
[00:11:56] [END OF AUDIO]
Copyright © 2022 New York Public Radio. All rights reserved. Visit our website terms of use at www.wnyc.org for further information.
New York Public Radio transcripts are created on a rush deadline, often by contractors. This text may not be in its final form and may be updated or revised in the future. Accuracy and availability may vary. The authoritative record of New York Public Radio’s programming is the audio record.